


View of an isolation ward for COVID-19 patients at the Command Hospital, Udhampur. Photo: PTI.
To tackle the COVID-19 pandemic, several countries have imposed restrictions on various activities to reduce the virus’s spread. These measures range from voluntary social distancing with public awareness campaigns to mandatorily shutting businesses and leisure activities, and prohibiting movement.
At first, the governments of various countries claimed that such measures, taken at the risk of economic disruption and dislocation, were necessary to flatten the curve, i.e. to keep too many people from getting infected at the same time so healthcare facilities aren’t overwhelmed, thus reducing the number of deaths.
But to our minds, this is not supported by scientific evidence or mathematical models of influenza epidemics. The scientific rationale for these measures is that healthcare infrastructure could be overwhelmed by a sharp rise in the number of cases requiring intensive clinical intervention, but there is no evidence that the number of deaths will drop. The assumption is that with care – specifically in-patient care in hospitals with critical care facilities and availability of physicians – the death rate is lower.
However, mathematical models don’t, and can’t, estimate how many lives are saved as a result of healthcare being available. Instead, such models take the case fatality rate as input and yield forecasts about how the number of cases might evolve. In epidemiology, the case fatality rate (CFR) is the proportion of people who die from a specified disease among all individuals diagnosed with the disease over a certain period of time. In effect, it’s a measure of the probability that a hospitalised COVID-19 patient will die. Its value varies with geography and in time, meaning it changes as the pandemic progresses. However, there is no estimated CFR if healthcare facilities such as hospital beds and physicians aren’t available.
In an attempt to investigate whether the availability of healthcare and doctors makes a difference to the outcomes of a COVID-19 infection, we plotted worldwide data on COVID-19 CFR against per capita availability of hospital beds and physicians.
Figure 1 shows hospital beds have a negligible, but beneficial, effect on reducing COVID-19 fatalities. To understand how small the effect is, consider the regression line: with nearly no hospital beds, the CFR is 4.7%, while with lots of beds (10 beds per 1,000 persons), the CFR drops only to 3.7%.

Figure 1: The countries towards the bottom report fewer COVID-19 fatalities. The countries marked in red have the higher COVID-19 CFR within an interval in the hospital-bed axis. The black dotted line is a linear trendline relating the data of countries marked in blue. The ISO code for countries marks the data points. Sources: ourworldindata.org for country-wise COVID-19 CFR and World Bank for country-wise hospital bed numbers.
India has 0.7 beds per 1,000 persons, so no reduction in COVID-19 CFR can be expected in India even if the lockdown has been used to provide extra medical facilities.
Figure 2 shows again that there is an insignificant correlation between the availability of physicians and COVID-19 CFR. Curiously, the CFR increases when there are more doctors. Again, consider the regression line: if there is a negligible number of doctors, the COVID-19 CFR is 3.9%, but if doctors are highly available (5 per 1,000 persons), the CFR could increase to 4%.
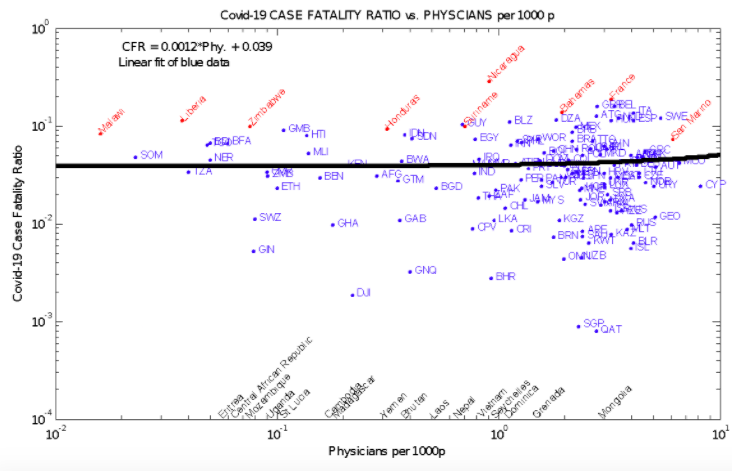
Figure 2: The countries towards the bottom report fewer COVID-19 fatalities. The countries marked in red have the higher COVID-19 CFR within an interval in the physician axis. The black dotted line is a linear trendline relating the data of countries marked in blue. The ISO code for countries marks the data points. Sources: ourworldindata.org for country-wise COVID-19 CFR and World Bank for country-wise hospital bed numbers.
India has 0.8 doctors per 1,000 persons, so – again – no reduction in COVID-19 CFR can be expected in India.
The above results show that protection against the new virus seems to be provided almost entirely by the body’s own immune system, rather than by doctors or ventilators. Specifically, the per capita availability of hospital beds and physicians are quantitative proxies for the quality of any healthcare delivery system, and assume public healthcare system availability for all.
Many countries have restricted citizens’ movement and imposed some nearly draconian measures, especially where there was little time for the people to prepare. The lockdown’s effects on lives, livelihoods and the economy were unpredictable but are slowly unfolding. India is particularly vulnerable, with one of the world’s lowest per capita public expenditures on health, and whose citizens pay out of pocket for care provided by for-profit institutions. Most of the population can’t access sophisticated critical care facilities.
If the purpose of a lockdown is to protect the lives of the few over the livelihoods of the rest, it’s logical to not overload ICUs and overuse ventilators. But even this limited premise is suspect, as the global COVID-19 CFR data indicated. Once a person becomes infected, it would seem the availability of beds, ventilators and physicians plays a small role in reducing the chances of dying.
Ajit Haridas is the former chief scientist of CSIR-NIIST Thiruvananthapuram and former chairman of the Kerala State Pollution Control Board.
Gangan Pratap is an aeronautical engineer and former scientist at the National Aeronautical Laboratory, Bangalore and former VC of Cochin University of Science and Technology. He is currently a professor at the A.P.J. Abdul Kalam Technological University, Thiruvananthapuram.