


A sanitation worker receives a dose of Covaxin at a hospital in New Delhi, February 16, 2021. Photo: PTI Photo/Manvender Vashist.
How can we make sense of India’s big fall in COVID-19 cases and deaths since September last year? This question is being asked a lot – in the media and on social media.
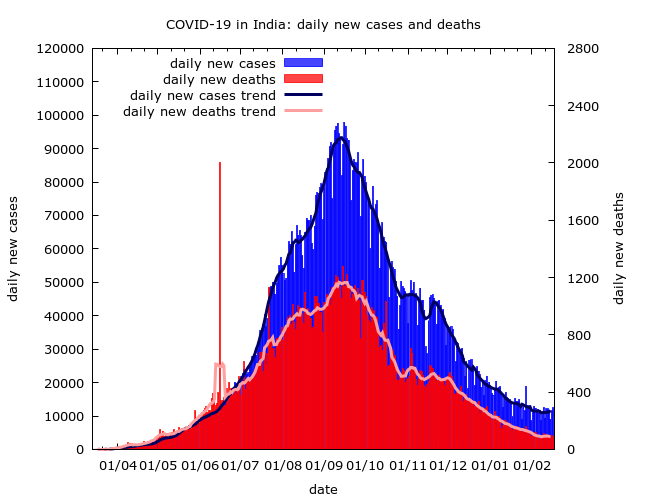
Lockdown after lockdown failed to reverse the rise in daily cases until finally, in August and September, the epidemics in several states with high case-loads began to slow. Nationally, the drop has been quite steady since then apart from some wobbles in November.
There are competing explanations for this trend, mainly around the themes of “successful control” and “herd immunity”. Are we seeing the result of effective policies or is the epidemic heading towards its natural conclusion? How could transmission slow so much when seroprevalence survey data says that fewer than one quarter of Indians have had the infection?
These are practically important questions because they tell us what the future might hold. COVID watchers asked similar questions after Pakistan’s first wave, before cases and deaths rose again. Across the world – including in several Indian cities – we’ve seen COVID-19 epidemics appear to run their course only to flare up again with surprising vigour. Are we seeing hints that India might be heading this way?
The decline is real but exaggerated
We cannot discuss COVID-19 cases without first noting that cases are recorded infections which, as we know from multiple serosurveys, are a small fraction of India’s total infections. Some areas pick up 10% or more of their infections in testing; others less than 1%.
Similarly, recorded COVID-19 deaths underestimate the epidemic’s true toll – but with high variability. The data is very incomplete, but it suggests that in some places the great majority of COVID-19 deaths have gone unrecorded.
Why does this matter? Because analyses based on case and death data alone can go very wrong. The 2021 Economic Survey, for example, is full of incorrect claims built solely around this data, heaping praise on states which failed to monitor their epidemics or fudged their data. When we see a fall in cases and recorded deaths it is correct to wonder if more infections are going unrecorded.
All the data taken together, including local reports and seroprevalence survey results, provides strong evidence that the national wind-down is real. Active infection nationwide has reduced a great deal since last September.
There is an important caveat though. It is likely that the scale of the improvement is less than it appears because as the wave receded disease moved increasingly to rural areas with weaker surveillance. Daily new cases have dropped by almost 90%, but the true drop in daily new infections is probably more modest.
What has driven the decline?
Mitigation
Let’s start with the basics. Active infections decline when, on average, one infected person infects fewer than one more. Chains of infection get broken faster than new ones are made. Many – though not all – possible reasons for this can be placed under two headings: “mitigation” and “immunity”.
Mitigation is used here to mean changes in behaviours and environments to cut down on disease-spreading events. Also called non-pharmaceutical interventions (NPIs), these may be voluntary or mandated. They may involve restricting gatherings, limiting travel, encouraging masks, or increasing ventilation in workplaces for example.
Mitigation has decreased over time, but has not gone away. Gatherings are still controlled, many educational institutions remain physically closed or partially open, public transport is still restricted in some areas, and masks are still encouraged.
Estimating the effect of such measures is difficult. How important, for example, are school and college closures in curbing spread, and what can we learn from school outbreaks? These are not easy questions – the role of transmission in schools is a topic of hot debate internationally, and the data is unclear.
Even without specific restrictions, many people and authorities are still being cautious. A recent cluster of cases in a Bengaluru apartment complex following a party, triggered increased precautions in the city. I imagine the residents considered the risks of this gathering before making their unfortunate decision. No doubt other associations have avoided such gatherings, whatever the rules may or may not permit.
Immunity
Mitigation reduces transmission by changing behaviours or environments; but transmission is also slowed by increasing levels of immunity.
We know that people can become immune to COVID-19 for some time through infection or vaccination. But India’s vaccination roll-out has so far been too limited in scale to contribute much to its COVID story. Immunity acquired through infection on the other hand has, without any doubt, played a part in slowing the disease. Is it sufficient to explain the national data?
This is a difficult question. If the disease is a fire, then those who are immune act like a fire retardant – a barrier between the fire and unspent fuel. Even without any mitigation, if the fraction of immune people reaches the so-called herd immunity threshold (HIT), the fire begins to die down. Or so the basic theory says.
But discussions of herd immunity are often too loose. It is an idealised mathematical notion based on simple assumptions which do not necessarily hold in the real world. To the extent that it makes sense, we find that:
* The natural speed of spread, and hence the estimated HIT, varies widely between states and even neighbourhoods. Herd immunity at national level would be a consequence of herd immunity locally, but must also take into account the movement of people between areas..
* Estimating HIT is difficult. The estimates often call on early data prior to mitigation; but such data is limited and from those areas where spread was first picked up. Early national data largely reflected a few urban hotspots where we expect spread to be quite rapid.
There are other complications. HITs may be lower in practice than in theory. A relatively small number of “super-spreaders” are associated with the majority of COVID-19 spread, partly for biological reasons. If many of these individuals tend to become infected, and hence immune, early in an outbreak – as some modelling suggests – this would rapidly slow transmission. This could be occurring to some extent, although city epidemics like Mumbai’s which refuse to die away despite high prevalence seem at odds with this theory.
Putting it all together
So, herd immunity is a complex notion and it is doubtful how far it explains national data. But there is little doubt that effective mitigation and increasing levels of immunity have combined to slow the epidemic. Could there be other factors at play?
In theory, yes. There could be seasonal or pollution-related effects. There could also be a drop in transmission if, for some reason, more and more people get asymptomatic disease, or a less contagious COVID-19 variant becomes prevalent. Note, however, that the new variants in the headlines are more, not less, contagious, and there isn’t convincing evidence of a big role for seasonality or reduced infectiousness at the moment.
My own guess is that the national picture is very varied. The HIT in some regions may indeed be considerably lower than the 60% figure often used. Some areas where spread has been relatively unchecked may be close to herd immunity. In others, mitigation is likely playing a key role in preventing resurgence.
This implies that if life truly returned to pre-pandemic settings we would see a surge in infections in many areas. Ironically, as Kerala’s late-starting epidemic demonstrated, regions with the most effective mitigation are most vulnerable to such a resurgence.
At the time of writing there are hints that a new wave could be developing, most clearly in Maharashtra, but possibly in neighbouring Gujarat and Madhya Pradesh too. It is too early to be sure if these upswings will develop into a national upswing – there is still hope that swift responses will be able to contain them.
All the data is from covid19india.org.
Murad Banaji is a mathematician with an interest in disease modelling.